Radiofrequency Ablation of Solitary Liver Metastasis
Radiofrequency Ablation of Solitary Liver Metastasis
Radiofrequency ablation (RFA) uses thermal energy to treat and palliate many lesions in the body. It is the gold standard for treating osteoid osteomas and is a useful technique for pain palliation in bone metastases and some primary bone tumors. It is also used to treat liver metastases, solitary or multiple, as well as lung and renal tumors.
Even with difficult-to-approach cases, by using a combination of gantry tilting, a tandem method and other similar techniques, it is usually possible to place an electrode within liver and lung lesions.
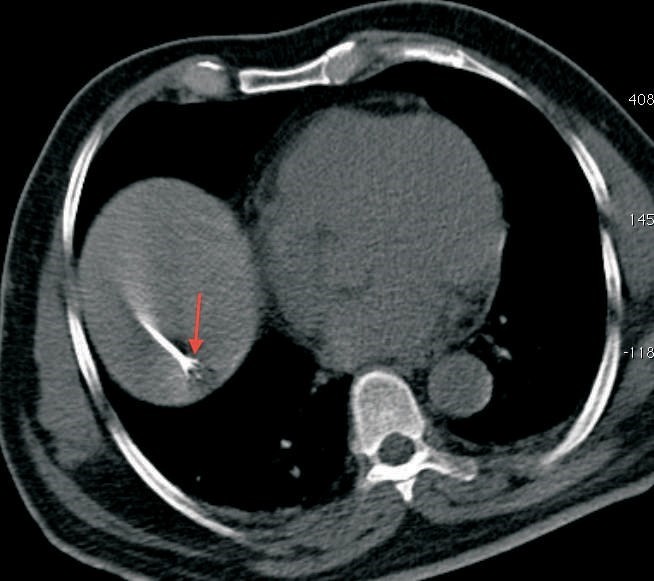
Recently we had an elderly gentleman with a solitary metastatic lesion (Fig. 1) measuring 1.2 cm in diameter in segment 7 of the liver, He had been operated earlier for carcinoma colon. We were able to safely introduce the RFA electrode into the lesion despite its deep location (Fig. 2), without puncturing the overlying pleura and lung, which were in the way. Since the lesion was close to the diaphragm, we had to take care to avoid puncturing the diaphragm. The lesion was ablated at 90 degrees for 7 ½ minutes and a good burn was achieved without any complications (Fig. 3).
RFA is indicated in liver metastases, typically as an alternative to surgical resection, either when resection is technically difficult, the patient is not a surgical candidate, or the patient has refused to undergo resection. If a good burn margin is achieved, the results are excellent.
Points:
- RFA is an established technique for treating liver metastases.
- It is indicated whenever resection is not feasible or possible.
- Even with difficult-to- approach lesions, a path can usually be found for electrode placement.